3 special nutrients of Remune™
Remune™ aims to increase the intake of polyunsaturated omega-3 fatty acids (especially EPA and DHA) and vitamin D together with energy and protein in order to supply patients with additional nutrients which they may not get in sufficient amounts through their normal diet.
Find more information about omega-3, whey protein and vitamin D and their special role as crucial nutrients in oncology.
Omega-3 from fish oil

What is omega-3?
Omega-3 polyunsaturated fatty acids (PUFAs) play an important role in cell membrane structure, fluidity and cell signaling. Omega-3 PUFAs, in particular eicosapentaenoic acid (EPA, C20:5 n-3) and docosahexaenoic acid (DHA, C22:6 n-3,) have been reported to have multiple effects.1 Omega-3 PUFAs are preferentially incorporated into cell membrane phospholipids, influence secondary messenger synthesis and modulate the expression of certain adhesion molecules at the surface of endothelial cells, monocytes and lymphocytes.2,3
The most abundant dietary PUFAs are omega-3 alpha linoleic acid (ALA, C18:3 n-3;) and the omega-6 linoleic acid (LA 18:2 n-6), most often ingested as plant oils. ALA is the direct precursor of EPA and DHA, but the conversion in humans is low, being in the range of 0.2% to 8% for ALA to EPA, <0.01% to 4% for ALA to DHA and 7% - 11% from EPA to DHA.4,5,6 Thus, EPA and DHA are commonly consumed as marine fatty acids from fatty cold water fish such as salmon or herring. In the enteral nutrition formulas, these fatty acids are present in the form of emulsified fish oil.7
Why is omega-3 (EPA & DHA) a special nutrient?
The human body has limited capacity to synthesize EPA and DHA.4,5,6 Supplementation of omega-3 PUFAs to the oral diet or in the setting of enteral nutrition could be useful for cancer patients because the potential of EPA and DHA was demonstrated for a number of cancer types in in vitro, animal and human studies.8,1
Possible effects could be9:
- regulation of apoptosis
- inhibition of cancer growth
- anti-angiogenic and antiproliferative effects
- anti-inflammatory and antithrombotic actions.
Possible clinical benefits of EPA and DHA supplementation* in cancer patients
- Stabilization or increase of body weight and lean body mass10-16
- Improved Quality of life (QoL)11,13,17
- Increased physical activity17
- Decreased resting energy expenditure (REE)18
- Immunomodulatory action and lower inflammation11
- Downregulation of acute-phase response reaction19
- Higher efficacy and lower adverse reactions of chemotherapy20,21
- Trend toward increase in overall survival21
*Data from fish oil capsules or ONS
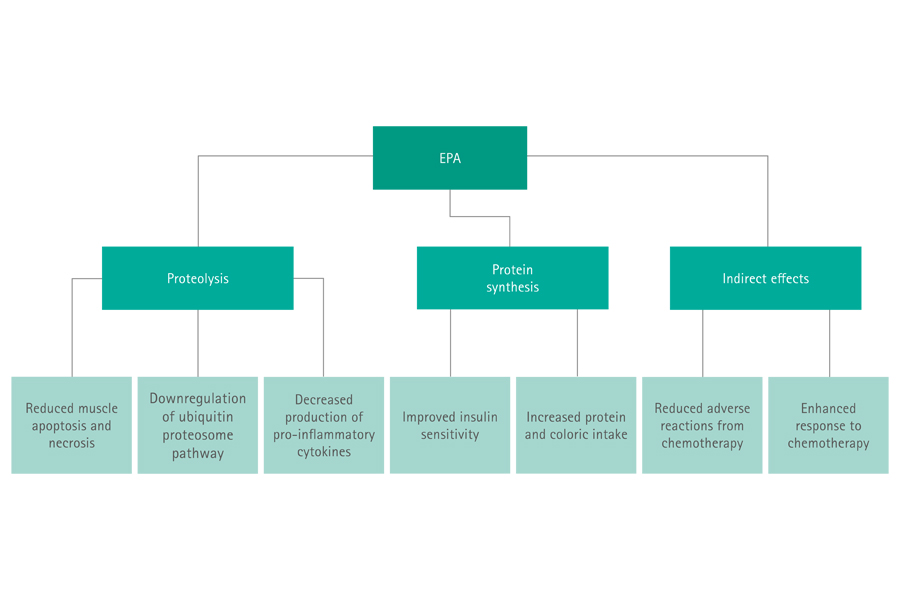
Studies suggest that EPA reduces tumor-induced proteolysis, stimulates the protein synthesis and has indirect effects like enhanced response to chemotherapy (see Fig. 1).16
Due the increasing evidence of benefit from omega-3 intervention in cancer patients, the 2017 ESPEN guideline for oncology states22:
„In patients with advanced cancer undergoing chemotherapy and at risk of weight loss or malnourished, we suggest to use supplementation with long-chain N-3 fatty acids or fish oil to stabilize or improve appetite, food intake, lean body mass and body weight.“
Even the 2009 ASPEN guideline for oncology stated23:
„Omega-3 Fatty acid supplementation may help stabilize weight in cancer patients on oral diets experiencing progressive, unintentional weight loss.“
Nutritional supplementation with omega-3 fatty acids from fish oil have shown several beneficial effects in cancer patients.
Whey protein

What is whey protein?
Whey protein accounts for about 20% of the total protein content of cow milk and counts to the high-quality proteins because of the amino acid content (high essential, branched-chain, and leucine amino acid amount).24,25
Whey protein can be extracted from the liquid byproduct from cheese manufacturing processes. It shows a high digestibility and quick absorption and thus can lead to higher concentrations of amino acids in blood immediately after meal and may result in higher muscle protein synthesis.26,27
Why is whey protein a special nutrient in oncology?
It is well known that oncology patients suffer from loss of muscle mass and inflammation.28 Therefore, whey protein became an interesting topic in the recent years.
Recent studies show that supplementation with whey protein in cancer patients can improve nutritional status.29,30 Intervention with whey protein in malnourished cancer patients undergoing chemotherapy resulted in improved body composition, muscle strength, and body weight.31 Studies showed also that whey protein could prevent or reduce severe toxicity during chemotherapy in colorectal or advanced cancer patients.29,31
The biological components of whey demonstrate immune-enhancing properties32 and may have specific anti-cancer effects.33 A recent meta-analysis conclude that whey protein may significantly reduce CRP among participants with high supplemental doses or increased baseline CRP levels.32
Whey protein as a dietary strategy on oncology became an interesting topic to increase muscle mass and strength, improve nutritional status, and reduce chemotherapy related toxicities.
Vitamin D

What is vitamin D?
Vitamin D is an essential vitamin important for calcium and phosphate homeostasis, bone metabolism and immune system.34 Since the last few years it is intensively discussed because of maintenance of muscle mass.35,36
Very few foods naturally contain vitamin D. These include oily fish such as salmon, mackerel and herring, mushrooms exposed to sunlight or that are sun-dried and cod liver oil. Sunlight exposure remains the major source of vitamin D for most children and adults.37
Vitamin D deficiency is associated with many acute and chronic illnesses including disorders of calcium metabolism, autoimmune diseases, some cancers, type 2 diabetes mellitus, cardiovascular disease and infectious diseases.37,38
The major circulating and active form of vitamin D in the body is 25 Hydroxy Vit D3 (short: 25-OH-D3).
Why is vitamin D a special nutrient?
Over the last years vitamin D is of special interest in the cancer world because vitamin D deficiency has been found to be associated with a variety of cancers, including prostate, multiple myeloma, colorectal and breast cancer. Vitamin D is believed to influence cancer prevalence, risk and survival.39
Cancer patients and concurrent low serum vitamin D 25 hydroxy levels show lower survival or higher cancer recurrence as cancer patients with normal Vitamin D 25 hydroxy levels.40,41,42 Moreover, the expression of vitamin D receptor in the majority of immune cells and the ability of these cells to actively metabolize vitamin D into its active form (25 hydroxy Vit D) shows the important role of vitamin D signaling in maintaining a healthy immune system.43 Inflammatory processes may link vitamin D to cancer survival.44
Vitamin D deficiency plays also a role in muscle weakness and fracture risk. While larger clinical trials of vitamin D supplementation are lacking in cancer patients, the evidence from clinical trials among older adults supports a possible benefit of vitamin D on muscle strength, fall and fracture reduction.45
Summary
Possible benefits of the 3 special nutrients in nutrition therapy of oncology patients
Omega-3 benefits
At a glance, the possible beneficial effects of omega-3 from fish oil could be:
- Stabilization or increase of body weight and lean body mass10-16
- Improved Quality of life (QoL)11,13,17
- Increased physical activity17
- Decreased resting energy expenditure (REE)18
- Immunomodulatory action and lower inflammation11
- Downregulation of acute-phase response reaction19
- Higher efficacy and lower adverse reactions of chemotherapy20,21
- Trend toward increase in overall survival21
Whey protein benefits
- Improved nutritional status29,30
- Improved body composition, muscle strength, and body weight31
- Prevention or reduction of severe toxicity during chemotherapy in colorectal or advanced cancer patients29,31
- The biological components of whey demonstrate immune-enhancing properties32 and may have specific anti-cancer effects33
- Reduction of CRP among participants with high supplemental doses (> 20 g/day) or increased baseline CRP levels32
Vitamin D benefits
At a glance, the possible beneficial effects of vitamin D could be:
- Influence of cancer prevalence, risk and survival39-42
- Inflammatory processes may link vitamin D to cancer survival44
- Improved muscle strength, fall and fracture reduction45
Download
Highlights


References
1 Laviano A, Rianda S, Molfino A, Rossi Fanelli F. Omega-3 fatty acids in cancer. Curr Opin Clin Nutr Metab Care. 2013;16(2):156-61.
2 Wahle KW, Rotondo D. Fatty acids and endothelial cell function: regulation of adhesion molecule and redox enzyme expression. Curr Opin Clin Nutr Metab Care. 1999;2:109–15.
3 Calder PC. N-3 polyunsaturated fatty acids and inflammation: from molecular biology to the clinic. Lipids. 2003;38:343–52.
4 Burdge GC, Calder PC. Conversion of a-linolenic acid to longer chain polyunsaturated fatty acids in human adults. Reprod Nutr Dev. 2005;45:581-97.
5 Arterburn LM, Hall EB, Oken H. Distribution, interconversion, and does response of n-3 fatty acids in humans. Am J Clin Nutr. 2006;83(suppl):1467-76.
6 Hussein N, Ah-Sing E, Wilkinson P, Leach C, Griffin BA, Millward DJ. Long-chain conversion of [13C]linoleic acid and alpha-linolenic acid in response to marked changes in their dietary intake in men. J Lipid Res. 2005; 46:269-80.
7 Simopoulos AP. Evolutionary aspects of diet and essential fatty acids. World Rev Nutr Diet. 2001;88:18-27.
8 Pappalardo G, Almeida A, Ravasco P. Eicosapentaenoic acid in cancer improves body composition and modulates metabolism. Nutrition. 2015;31(4):549-555.
9 Fabian CJ, Kimler BF, Hursting SD. Omega-3 fatty acids for breast cancer prevention and survivorship. Breast Cancer Res. 2015;17(1):62.
10 Barber MD, Ross JA, Voss AC, Tisdale MJ, Fearon KC. The effect of an oral nutritional supplement enriched with fish oil on weight-loss in patients with pancreatic cancer. Br J Cancer. 1999;81(1):80-6.
11 de Aguiar Pastore Silva J, Emilia de Souza Fabre M, Waitzberg DL. Omega-3 supplements for patients in chemotherapy and / or radiotherapy: A systematic review. Clin Nutr. 2015;34(3):359-66.
12 Read JA, Beale PJ, Volker DH, Smith N, Childs A, Clarke SJ. Nutrition intervention using an eicosapentaenoic acid (EPA)-containing supplement in patients with advanced colorectal cancer. Effects on nutritional and inflammatory status: a phase II trial. Support Care Cancer. 2007;15(3):301-7.
13 Trabal J, Leyes P, Forga M, Maurel J. Potential usefulness of an EPA-enriched nutritional supplement on chemotherapy tolerability in cancer patients without overt malnutrition. Nutr Hosp. 2010;25(5):736-40.
14 van der Meij BS, Langius JA, Smit EF, Spreeuwenberg MD, von Blomberg BM, Heijboer AC, et al. Oral nutritional supplements containing (n-3) polyunsaturated fatty acids affect the nutritional status of patients with stage III non-small cell lung cancer during multimodality treatment. J Nutr. 2010;140(10):1774-80.
15 Sanchez-Lara K, Turcott JG, Juarez-Hernandez E, Nunez-Valencia C, Villanueva G, Guevara P, et al. Effects of an oral nutritional supplement containing eicosapentaenoic acid on nutritional and clinical outcomes in patients with advanced non-small cell lung cancer: randomised trial. Clin Nutr. 2014;33(6):1017-23.
16 Murphy RA, Yeung E, Mazurak VC, Mourtzakis M. Influence of eicosapentaenoic acid supplementation on lean body mass in cancer cachexia. Br J Cancer. 2011;105(10):1469-73.
17 van der Meij BS, Langius JA, Spreeuwenberg MD, Slootmaker SM, Paul MA, Smit EF, et al. Oral nutritional supplements containing n-3 polyunsaturated fatty acids affect quality of life and functional status in lung cancer patients during multimodality treatment: an RCT. Eur J Clin Nutr. 2012;66(3):399-404.
18 Moses AW, Slater C, Preston T, Barber MD, Fearon KC. Reduced total energy expenditure and physical activity in cachectic patients with pancreatic cancer can be modulated by an energy and protein dense oral supplement enriched with n-3 fatty acids. Br J Cancer. 2004;90(5):996-1002.
19 Wigmore SJ, Fearon KC, Maingay JP, Ross JA. Downregulation of the acute-phase response in patients with pancreatic cancer cachexia receiving oral eicosapentaenoic acid is mediated via suppression of interleukin-6. Clin Sci (Lond). 1997;92(2):215-21.
20 Bougnoux P, Hajjaji N, Ferrasson MN, Giraudeau B, Couet C, Le Floch O. Improving outcome of chemotherapy of metastatic breast cancer by docosahexaenoic acid: a phase II trial. Br J Cancer. 2009;101(12):1978-85.
21 Murphy RA, Mourtzakis M, Chu QS, Baracos VE, Reiman T, Mazurak VC. Supplementation with fish oil increases first-line chemotherapy efficacy in patients with advanced nonsmall cell lung cancer. Cancer. 2011;117(16):3774-80.
22 Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, Bozzetti F et al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr. 2017;36(1):11–48.
23 August DA, Huhmann MB. A.S.P.E.N. clinical guidelines: nutrition support therapy during adult anticancer treatment and in hematopoietic cell transplantation. JPEN J Parenter Enteral Nutr. 2009; 33(5):472-500.
24 Devries MC, Phillips SM. Supplemental protein in support of muscle mass and health: advantage whey. J Food Sci. 2015;80 Suppl 1:A8-a15.
25 Marshall K. Therapeutic applications of whey protein. Altern Med Rev. 2004;9(2):136-56.
26 Luiking YC, Deutz NE, Memelink RG, Verlaan S, Wolfe RR. Postprandial muscle protein synthesis is higher after a high whey protein, leucine-enriched supplement than after a dairy-like product in healthy older people: a randomized controlled trial. Nutr J. 2014;13:9.
27 Chanet A, Verlaan S, Salles J, Giraudet C, Patrac V, Pidou V, et al. Supplementing Breakfast with a Vitamin D and Leucine- Enriched Whey Protein Medical Nutrition Drink Enhances Postprandial Muscle Protein Synthesis and Muscle Mass in Healthy Older Men. J Nutr. 2017;147(12):2262-71.
28 Arends J, Baracos V, Bertz H, Bozzetti F, Calder PC, Deutz NEP, et al. ESPEN expert group recommendations for action against cancer-related malnutrition. Clin Nutr. 2017;36(5):1187-1196.
29 Mazzuca F, Roberto M, Arrivi G, Sarfati E, Schipilliti FM, Crimini E, et al. Clinical Impact of Highly Purified, Whey Proteins in Patients Affected With Colorectal Cancer Undergoing Chemotherapy: Preliminary Results of a Placebo-Controlled Study. Integr Cancer Ther. 2019;18:1534735419866920.
30 Ren G, Zhang J, Li M, Yi S, Xie J, Zhang H, et al. Protein blend ingestion before allogeneic stem cell transplantation improves protein-energy malnutrition in patients with leukemia. Nutr Res. 2017;46:68-77.
31 Cereda E, Turri A, Klersy C, Cappello S, Ferrari A, Filippi AR, et al. Whey protein isolate supplementation improves body composition, muscle strength, and treatment tolerance in malnourished advanced cancer patients undergoing chemotherapy. Cancer Med. 2019;8(16):6923-6932.
32 Zhou LM, Xu JY, Rao CP, Han S, Wan Z, Qin LQ. Effect of whey supplementation on circulating C-reactive protein: a metaanalysis of randomized controlled trials. Nutrients. 2015;7(2):1131-43.
33 Teixeira FJ, Santos HO, Howell SL, Pimentel GD. Whey protein in cancer therapy: A narrative review. Pharmacol Res. 2019;144:245-256.
34 Ross AC, Taylor CL, Yaktine AL et al. Dietary Reference Intakes for Calcium and Vitamin D. Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Available from: https://www.ncbi.nlm.nih.gov/books/NBK56061/: Washington (DC): National Academies Press (US); 2011.
35 Girgis CM. Vitamin D and Skeletal Muscle: Emerging Roles in Development, Anabolism and Repair. Calcif Tissue Int. 2020;106(1):47-57.
36 Montenegro KR, Cruzat V, Carlessi R, Newsholme P. Mechanisms of vitamin D action in skeletal muscle. Nutr Res Rev. 2019;32(2):192-204..
37 Holick MF. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev Endocr Metab Disord. 2017;18(2):153-65.
38 Wacker M, Holick MF. Vitamin D - effects on skeletal and extraskeletal health and the need for supplementation. Nutrients. 2013;5(1):111-48.
39 Gupta D, Vashi PG, Trukova K, Lis CG, Lammersfeld CA. Prevalence of serum vitamin D deficiency and insufficiency in cancer: Review of the epidemiological literature. Exp Ther Med. 2011;2(2):181-93.
40 Maalmi H, Walter V, Jansen L, Boakye D, Schottker B, Hoffmeister M, et al. Association between Blood 25-Hydroxyvitamin D Levels and Survival in Colorectal Cancer Patients: An Updated Systematic Review and Meta-Analysis. Nutrients. 2018;10(7):896.
41 Vaughan-Shaw PG, Zgaga L, Ooi LY, Theodoratou E, Timofeeva M, Svinti V, et al. Low plasma vitamin D is associated with adverse colorectal cancer survival after surgical resection, independent of systemic inflammatory response. Gut 2020;69:103-111.
42 Fuchs MA, Yuan C, Sato K, Niedzwiecki D, Ye X, Saltz LB, et al. Predicted vitamin D status and colon cancer recurrence and mortality in CALGB 89803 (Alliance). Ann Oncol. 2017;28(6):1359-67.
43 El-Sharkawy A, Malki A. Vitamin D Signaling in Inflammation and Cancer: Molecular Mechanisms and Therapeutic Implications. Molecules. 2020;25(14):E3219.
44 van Harten-Gerritsen AS, Balvers MG, Witkamp RF, Kampman E, van Duijnhoven FJ. Vitamin D, Inflammation, and Colorectal Cancer Progression: A Review of Mechanistic Studies and Future Directions for Epidemiological Studies. Cancer Epidemiol Biomarkers Prev. 2015;24(12):1820-1828.
45 Bischoff-Ferrari H. Relevance of vitamin D in bone and muscle health of cancer patients. Anticancer Agents Med Chem. 2013;13(1):58-64.